

Por Flor Ortiz. Medica Veterinaria Zootecnista (FMVZ-UNAM), investigadora médica del uso medicinal del cannabis en medicina veterinaria y humana.

Las personas de la tercera edad son pacientes con necesidades especiales, sin duda un grupo que puede obtener beneficios del cannabis o marihuana medicinal. El cannabis puede ayudar a tratar a los adultos mayores con menos riesgos que muchos medicamentos actuales.
Actualmente, el cannabis o marihuana medicinal se está introduciendo rápidamente en el arsenal farmacológico, incluyéndose su uso en los pacientes de edad avanzada. Debido a las características únicas de la población geriátrica, existe la necesidad de medicamentos seguros para abordar sus dolencias.
El cannabis medicinal ha demostrado ser prometedor para tratar muchas afecciones que preocupan a los pacientes de edad avanzada, por lo que revisaremos el potencial terapéutico actual del cannabis en esta población. [8]
Población geriátrica en México
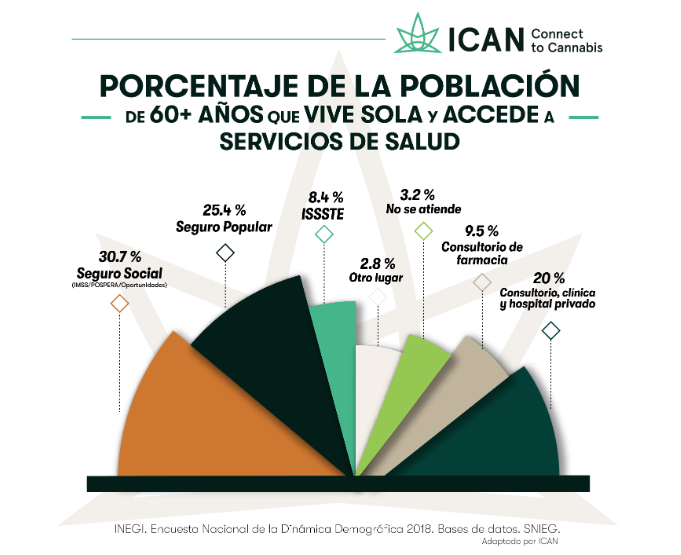
Con base en la Encuesta Nacional de la Dinámica Demográfica (ENADID) 2018, en el país residen 15.4 millones de personas de 60 años o más, de las cuales 1.7 millones viven solas. Casi la mitad de los adultos mayores (47.9 %) vive en hogares formados por un solo núcleo familiar, y 11.4 % viven solos. Siete de cada diez adultos mayores que viven solos presentan algún tipo de discapacidad o limitación.
En el país, 85.4 % de las personas de edad avanzada que viven solas están afiliadas a una institución de servicios de salud, y la mayoría de ellas buscan atención médica cuando tienen un problema de salud. De hecho, 9 de cada 100 se atienden en el consultorio de una farmacia.

ICAN® Todos los derechos reservados. No se permite la modificación de las imágenes ni los textos aquí contenidos. Se permite su reproducción sin modificación cuando se cite a ICAN como autor y se enlace a www.ican.mx y/o al Facebook @ICANvets. Diseño: Zaira Orozco
El deterioro natural de las funciones del cuerpo debido al envejecimiento dificulta el desempeño de las actividades de la vida diaria y se manifiesta principalmente por la pérdida gradual de la independencia física. Los adultos mayores tienen mayor riesgo de sufrir alguna discapacidad o limitación y, por lo tanto, necesitar algún tipo de ayuda o asistencia. En el caso de quienes viven solos, es muy probable que no cuenten con alguna ayuda inmediata o cercana para realizar sus actividades diarias o en algunos casos, requieran de cuidados específicos. [7]
ICAN® Todos los derechos reservados. No se permite la modificación de las imágenes ni los textos aquí contenidos. Se permite su reproducción sin modificación cuando se cite a ICAN como autor y se enlace a www.ican.mx y/o al Facebook @ICANvets. Diseño: Zaira Orozco
Los datos epidemiológicos muestran que la población de mayor edad constituye un segmento creciente de usuarios de cannabis medicinal, que varía aproximadamente del 7 % al 33 % dependiendo del país. [1] En un estudio reciente realizado en Israel, se encontró que de 279 pacientes con cáncer que recibían cannabis medicinal, el 50 % tenían 60 años o más, lo cual da pie para poner atención en este segmento poblacional como posibles pacientes de la medicina cannábica. [8]
Cannabis como alternativa a otros medicamentos
El manejo de diferentes síntomas en los adultos mayores puede ser un desafío, ya que los medicamentos convencionales pueden causar efectos secundarios que empeoran la calidad de vida u ocasionan otros síntomas. Por mencionar algunos ejemplos: los opioides pueden aumentar el riesgo de estreñimiento, confusión, caídas y fracturas; las benzodiacepinas también aumentan el riesgo de fracturas y lesiones en los tejidos blandos; los antagonistas de la dopamina pueden aumentar el riesgo de muerte en adultos mayores con demencia.
Debido a estos problemas con el arsenal actual de intervenciones sintomáticas y los efectos secundarios de los fármacos utilizados de manera común, los cannabinoides pueden ofrecer una alternativa para ayudar a los adultos mayores. [4] Muchos de los síntomas en estos pacientes pueden no estar adecuadamente controlados por los tratamientos farmacológicos convencionales, ya sea debido a los efectos subóptimos de las farmacoterapias o los efectos adversos inaceptables de éstas. [11]
Áreas de aplicación del cannabis en geriatría
Las preparaciones de cannabis contienen numerosos cannabinoides, incluidos delta-9-tetrahidrocannabinol (THC) y cannabidiol (CBD), como sus principales componentes. Estos cannabinoides actúan sobre un sistema cannabinoide endógeno. [12] El tratamiento con cannabis medicinal puede brindar ayuda a los adultos mayores en áreas como: disminución del dolor, mejor calidad del sueño, cambios motores como disminución de temblores o espasticidad, y mejoría en las alteraciones del estado de ánimo y agitación. [11]
Existe evidencia sustancial que sugiere que la actividad del sistema endocannabinoide (SEC) disminuye durante el envejecimiento, ya que la cantidad de receptores, endocannabinoides y proteínas se reduce con el paso del tiempo. Por esto, la restauración de las señales del SEC en individuos de edad avanzada podría ser una estrategia efectiva para tratar las deficiencias cognitivas relacionadas con la edad. [3]
Los principales síntomas o enfermedades para los que se ha empleado el cannabis para ayudar a los adultos mayores son los siguientes: [1,5,8,11,12]
-
Enfermedades articulares.
-
Enfermedad de Parkinson.
-
Dolor crónico.
-
Demencia y Alzheimer.
-
Enfermedades neurológicas y psiquiátricas.
-
Alteraciones del sueño.
-
Náusea y vómito (asociados a quimioterapia).
-
Enfermedades respiratorias.
-
Desórdenes del estado de ánimo y agitación.
Las formas más comunes de uso en este grupo etario son: la aplicación tópica, la pulverización o aplicación de spray debajo de la lengua, seguidas por la ingestión de cápsulas, el vapeo y finalmente los comestibles. [6]
Consideraciones para el uso y aplicación de la medicina cannabinoide en geriatría
Los datos sobre eficacia y seguridad establecidos en estudios con adultos no pueden simplemente extrapolarse al grupo de pacientes mayores. Adicionalmente, la alta prevalencia de comorbilidad y polifarmacia relacionada a los pacientes geriatras complica aún más el tratamiento farmacológico en esta población. Por lo tanto, es muy relevante estudiar los efectos de los cannabinoides en pacientes mayores por separado, antes de recomendar el uso generalizado. [12]
Es importante tomar las siguientes consideraciones:
-
Evaluar el historial psiquiátrico y de abuso de sustancias en cualquier paciente al que se quiera recomendar el tratamiento con cannabis, en particular si se desea prescribir alguna formulación que contenga THC.
-
Evaluar si existen trastornos cognitivos antes de recomendar el cannabis medicinal, pues el riesgo de deterioro cognitivo aumenta con la edad.
-
El cannabis (en especial el THC) puede perjudicar la habilidad para conducir, por lo que se debe advertir a las personas que no conduzcan durante al menos 6 horas después de vaporizar o fumar y 9 horas después de consumir comestibles.
El abuso de marihuana no ha sido históricamente una preocupación importante en los adultos mayores, sin embargo, es posible que se pueda relacionar a un mayor abuso de sustancias (de todas las variedades) en los adultos mayores. [4]
Seguridad y efectos adversos en pacientes geriatras
Determinar la seguridad del tratamiento y la dosis es un desafío para los médicos. Por lo tanto, se aconseja que se proceda con precaución con la dosificación siguiendo la regla “comience bajo y vaya lento”, hasta alcanzar una dosis que tenga un efecto sobre los síntomas.
Al comenzar un tratamiento cannabinoide, se requiere una titulación lenta de la dosis para evitar efectos adversos, incluidas las caídas y la hipotensión ortostática. [9] Adicionalmente, se recomienda hacer un seguimiento del paciente para monitorearlo en busca de falta de respuesta al tratamiento, complicaciones o abuso, mal uso o desvío. [2]
Los efectos adversos comunes que experimentan los pacientes debido al consumo de cannabis incluyen: mareos, euforia, somnolencia, confusión y desorientación. Estos eventos son particularmente importantes en la población de edad avanzada, ya que pueden sufrir afecciones como demencia, caídas frecuentes, problemas de movilidad, discapacidad auditiva o visual. [1]
La toxicidad aguda y la sobredosis también son posibles con el consumo de marihuana medicinal, en especial en pacientes que no han sido evaluados por un médico y no siguen un régimen para su dosificación. El autoconsumo sin indicaciones médicas podría llevar a una variedad de efectos no deseados. Además, existen diferencias farmacocinéticas según la vía de administración. [10]
Los productos por vía oral pueden tardar hasta seis horas después de la ingestión en ser absorbidos, lo que puede llevar a los usuarios a ingerir una dosis adicional antes de que los efectos clínicos se hayan presentado por completo, lo que aumenta el potencial de una sobredosis accidental. [10]
El efecto clínico más comúnmente reportado es la depresión respiratoria, pero también se ha informado de toxicidad cardiovascular y neurológica. La mayor disponibilidad de formulaciones comestibles a través de dispensarios ha llevado a más informes de ingestas más allá de la dosis recomendada. El consumo de grandes dosis únicas de THC puede desencadenar un episodio de psicosis aguda.
Interacciones medicamentosas para tomar en cuenta
Existe una alta sospecha de interacción farmacológica porque los cannabinoides son metabolizados por las enzimas CYP3A4, CYP2C9 y CYP2C19, involucradas en el metabolismo de numerosos medicamentos utilizados por los adultos mayores. Por lo anterior, las interacciones son posibles, por lo que se debe conocer la lista completa de los medicamentos que el paciente toma antes de que se puedan recetar los cannabinoides.
Conclusiones
En una encuesta realizada en 2020 a un grupo de pacientes en cuidados paliativos, se observó que solo el 29 % de los pacientes usaron THC antes del inicio de su enfermedad, y ninguno había usado CBD antes de su diagnóstico. Esto sugiere que los pacientes están buscando la medicina cannabinoide debido a sus beneficios percibidos sobre las enfermedades crónicas.
A pesar del aumento significativo en el uso del cannabis medicinal en personas de la tercera edad, la evidencia actual sobre la eficacia y seguridad del cannabis medicinal y cómo ayuda a los adultos mayores es escasa todavía. Más investigaciones al respecto nos permitirán comprender los efectos fisiológicos de los cannabinoides en las poblaciones de pacientes geriátricos y de cuidados paliativos, para poder orientar mejor sus aplicaciones clínicas.
Red de Médicos
ICAN te invita a conocer nuestra Red de Médicos capacitados en el uso de cannabis medicinal en México. Contamos con médicos que pueden prescribir medicamento con CBD seguro y legal, y también podrás encontrar veterinarios que pueden ayudar a nuestros amigos de cuatro patas.
Referencias
-
Abuhasira, R., Schleider, L. B.-L., Mechoulam, R., y Novack, V. (2018). Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly. European Journal of Internal Medicine, 49, 44–50. doi:10.1016/j.ejim.2018.01.019
-
Beauchet, O. (2018). Medical Cannabis use in older patients: update on medical knowledge. Maturitas.doi:10.1016/j.maturitas.2018.10.010
-
Bilkei-Gorzo, A., Albayram, O., Draffehn, A., Michel, K., Piyanova, A., Oppenheimer, H. Zimmer, A. (2017). A chronic low dose of Δ9-tetrahydrocannabinol (THC) restores cognitive function in old mice. Nature Medicine, 23(6), 782–787.doi:10.1038/nm.4311
-
Briscoe, J., y Casarett, D. (2018). Medical Marijuana Use in Older Adults. Journal of the American Geriatrics Society, 66(5), 859–863. doi:10.1111/jgs.15346
-
Häuser, W., Fitzcharles, M. A., Radbruch, L., y Petzke, F. (2017). Cannabinoids in Pain Management and Palliative Medicine. Deutsches Arzteblatt international, 114(38), 627–634. https://doi.org/10.3238/arztebl.2017.0627
-
Highet, B. H., Lesser, E. R., Johnson, P. W., y Kaur, J. S. (2020). Tetrahydrocannabinol and Cannabidiol Use in an Outpatient Palliative Medicine Population. American Journal of Hospice and Palliative Medicine®. https://doi.org/10.1177/1049909119900378
-
Instituto Nacional de Estadística y Geografía. (2019, septiembre 30). ESTADÍSTICAS A PROPÓSITO DEL DÍA INTERNACIONAL DE LAS PERSONAS DE EDAD (1º DE OCTUBRE). DATOS NACIONALES [Comunicado de prensa]. Recuperado de <PDF>, última consulta 20 julio de 2020.
-
Katz, I., Katz, D., Shoenfeld, Y., y Porat-Katz, B. S. (2017). Clinical Evidence for Utilizing Cannabinoids in the Elderly. The Israel Medical Association journal: IMAJ, 19(2), 71–75.
-
MacCallum, C. A., Russo, E. B. (2018). Practical considerations in medical cannabis administration and dosing. European Journal of Internal Medicine, 49, 12–19. doi:10.1016/j.ejim.2018.01.004
-
Mahvan, T., Hilaire, M., Mann, A., Brown, A., Linn, B., Gardner, T., y Lai, B. (2017). Marijuana Use in the Elderly: Implications and Considerations. The Consultant Pharmacist, 32(6), 341–351.doi:10.4140/tcp.n.2017.341
-
Minerbi, A., Häuser, W., y Fitzcharles, M.-A. (2018). Medical Cannabis for Older Patients. Drugs & Aging.doi:10.1007/s40266-018-0616-5
-
Van den Elsen, G. A. H., Ahmed, A. I. A., Lammers, M., Kramers, C., Verkes, R. J., van der Marck, M. A., y Rikkert, M. G. M. O. (2014). Efficacy and safety of medical cannabinoids in older subjects: A systematic review. Ageing Research Reviews, 14, 56–64.doi:10.1016/j.arr.2014.01.007

